The shoulder joint is the most mobile joint in the human body. All types of movements are possible in it: flexion-extension, abduction-adduction, supination-pronation, rotation. The price for such freedom of movement is the significant "fragility" of this joint. This article will focus on the most common injury trapped in athletes, systematically overloading the shoulder joints. This is a dislocated shoulder. In addition to the injury itself, we will touch on the issues of anatomy, biomechanics, first aid and, most importantly, preventive measures.
Shoulder anatomy
The shoulder joint is directly formed by the head of the humerus and the glenoid cavity of the scapula. The articular surfaces of the designated bones do not have absolute congruence. Simply put, they are not perfectly adjacent to each other. This moment is compensated for by a large formation called the articular lip. This is a cartilaginous body, adjacent, on the one hand, to the glenoid cavity of the scapula, and on the other, to the head of the humerus. The area of the glenoid lip is much larger than that of the articular surface of the scapula, which provides a better fit of the articulating surfaces inside the joint.

© Alila Medical Media - stock.adobe.com
The head of the humerus and the glenoid cavity of the scapula are covered with hyaline cartilage.

© designua - stock.adobe.com
Joint capsule and clavicle
Above the described structure is covered by a thin articular capsule. It is a sheet of connective tissue covering the anatomical neck of the humerus on one side, and the entire circumference of the glenoid cavity of the scapula on the other. The fibers of the coracohumeral ligament, tendons of the muscles that form the so-called rotator cuff of the shoulder are also interwoven into the tissue of the capsule. These include the infraspinatus, supraspinatus, large round and subscapularis muscles.
These elements strengthen the shoulder capsule. The muscles that make up the rotator cuff provide a certain amount of movement (read more about this below). Taken together, this formation limits the immediate joint cavity.

© bilderzwerg - stock.adobe.com
The clavicle also plays an important functional role in the structure of the shoulder joint. Its distal end is attached to the acromion or acromial process of the scapula. When the shoulder is abducted above an angle of 90 degrees, further movement occurs due to the mutual movement of the clavicle, the lower pole of the scapula and the chest. Looking ahead, we also say that the main muscle serving the shoulder joint - the deltoid - is attached to the described anatomical complex.
Rotator muscles
The condition of the muscles surrounding the joint is important for the health of the joint. (This statement applies to all joints in the human body, not just the shoulder). Let us repeat that the muscles serving the shoulder joint are located, so to speak, in two layers. The already mentioned muscles - rotators - belong to the deep one:
- infraspinatus - located on the body of the scapula, as it is not difficult to guess from the name, under its axis and is responsible for the supination of the shoulder;
- supraspinatus - located above the axis, participates in the abduction of the shoulder from the body. The first 45 degrees of abduction are performed primarily by the supraspinatus muscle;
- subscapularis - located on the front surface of the body of the scapula (between the scapula and the chest) and is responsible for performing supination of the head of the humerus;
- large round - runs from the lower pole of the scapula to the head of the humerus, is woven into the capsule by a tendon. Together in the infraspinatus muscle, pronates the shoulder.

© bilderzwerg - stock.adobe.com
Moving muscles
The tendons of the biceps and triceps brachii pass over the joint capsule. Since they are thrown over the head of the humerus, attaching to the acromial process of the scapula, these muscles also provide certain movements in the shoulder joint:
- biceps flexes the shoulder, bringing the body of the humerus at 90 degrees to the upper shoulder girdle;
- the triceps, together with the posterior head of the deltoid muscle, extends the shoulder, drawing the body of the humerus back relative to the body of the scapula;

© mikiradic - stock.adobe.com
It should be noted that the pectoralis major and minor muscles and the latissimus dorsi muscles are also attached to the articular tubercles of the humerus, providing appropriate movements:
- pectoralis major and minor - are responsible for bringing the humeral bones to each other;
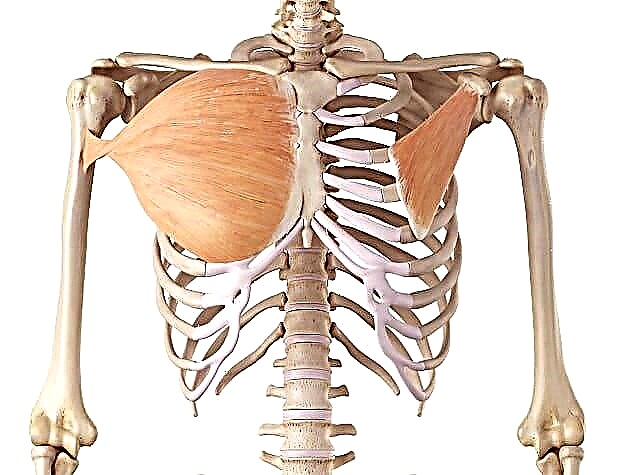
© Sebastian Kaulitzki - stock.adobe.com. Large (left) and small (right) pectoral muscles
- the broadest muscles of the back provide the movement of the bodies of the humeral bones downward in the frontal plane.
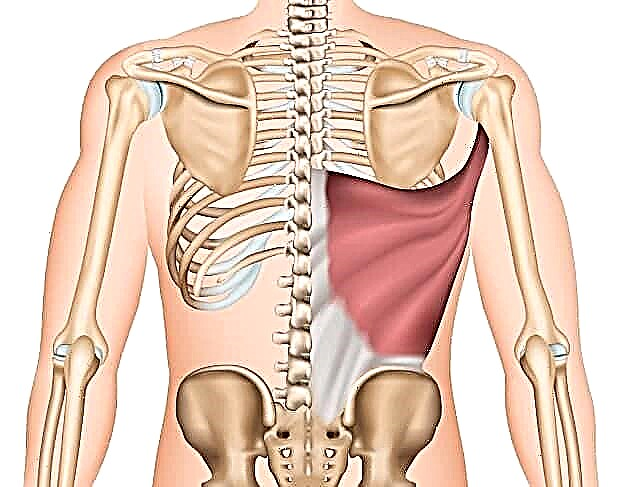
© bilderzwerg - stock.adobe.com. Latissimus muscle


The deltoid muscle is directly responsible for the movements in the shoulder joint. It has the following attachment points:
- the axis of the scapula is the starting point of the posterior portion of the deltoid muscle;
- acromion - the attachment point of the middle portion of the deltoid muscle;
- the acromial end of the clavicle is the attachment point of the anterior portion of the deltoid muscle.
Each serving, in fact, performs a different function, but balanced movement in the shoulder joint requires the coordinated work of all three "bundles". This is emphasized by the fact that all three bundles of the delta converge into a single tendon attached to the deltoid tuberosity of the humerus.
A large volume of these muscles provides an appropriate range of motion. However, in practice, they are the "base" of the joint. There is no reliable bone structure in the shoulder, which is why in the course of sports activities, especially when making amplitude movements, the shoulder joint is injured.
Mechanism of injury
Dislocation of the shoulder is the displacement of the head of the humerus relative to the glenoid cavity of the scapula. In the direction of displacement, several types of shoulder dislocation are distinguished.
Anterior dislocation
This type of injury occurs most easily, since it is the posterior pole of the humerus capsule that is least strengthened by tendons and ligaments. In addition, the posterior portion of the deltoid head must provide stability. However, it is not sufficiently developed among the overwhelming majority of ordinary people, and athletes are no exception.
This injury can occur under the action of a jerk effect on the limb - when practicing martial arts, performing elements on the rings, or on the uneven bars, the starting point of entering the handstand. Anterior dislocation is also possible as a result of a blow to the shoulder joint area, when practicing percussion martial arts (boxing, MMA, karate), or when landing, after performing a jumping element (workout, parkour).
Posterior dislocation
Posterior shoulder dislocationand withit is emitted not as often as the front, but, nevertheless, quite often in percentage. In this case, the head of the humerus is displaced to the rear of the glenoid cavity of the scapula. As you might guess, such a displacement of the head of the shoulder occurs when the anterior pole of the capsule of the shoulder joint is injured. Most often, the shoulder is in a flexion position, the arms are in front of you. Impact occurs in the distal part of the hand. Simply put, in the palm of your hand. Such an effect is possible when falling on outstretched arms, for example, with insufficient technical performance of the burpee exercise. Or, if the weight of the bar is not distributed correctly when performing the bench press.

© Alila Medical Media - stock.adobe.com
Lower dislocation
In inferior dislocation, the head of the humerus is displaced under the glenoid cavity of the scapula. This type of injury is not common and occurs with the arm raised up. Such an injury is possible when performing the "flag" exercise, when walking on hands, snatch and clean and jerk. The jerk and push, in this case, are the most traumatic, since the shoulders are in an anatomically unfavorable position, and the load falls vertically.
Habitual dislocation
There are other types of shoulder dislocations, but they are, in essence, combinations of the above types of the described injury.
The most unpleasant consequence of a shoulder dislocation is its chronicity - the formation of a habitual dislocation. This condition is characterized by the fact that any minimal impact on the previously affected joint is enough for the occurrence of a full-fledged dislocation. Most often, this pathology develops with improper treatment of the primary dislocation of the shoulder.
Dislocation signs and symptoms
The following unpleasant symptoms indicate an injury to the shoulder joint, namely, a dislocation:
- Sharp pain in the area of the damaged joint, accompanied by a kind of "wet crunch".
- Inability to make active movement in any of the axes of mobility of the shoulder joint.
- Characteristic displacement of the head of the humerus. In the deltoid region, the acromial process of the clavicle is determined, underneath is the "depression". (In case of inferior dislocation, the arm remains raised up, the head of the humerus can be felt in the chest area, armpit). The area itself, in comparison with a healthy one, looks "sunken". In this case, the affected limb becomes relatively longer.
- Swelling of the affected joint area. It develops due to traumatic damage to the vessels surrounding the joint area. The poured blood soaks into soft tissues, sometimes forming a rather large hematoma, which brings additional painful sensations. Moreover, you will not see the "blueing" of the deltoid area immediately after the injury - the subcutaneous vessels are damaged extremely rarely, and the visible hematoma is characteristic only for the direct injury of the indicated vessels.
First aid for dislocated shoulder
Below are some tips that will come in handy if you have to provide first aid to the victim.
No need to try to straighten your shoulder yourself !!! In no case! Inexperienced attempts at self-reduction of the shoulder lead to injuries of the neurovascular bundle and serious ruptures of the shoulder capsule!
First, you need to fix the limb, ensuring its maximum rest and limitation of mobility. If there is a pain reliever (analgin, ibuprofen or diclofenac and the like), it is necessary to give medicine to the victim in order to reduce the severity of the pain syndrome.
If ice, snow, frozen dumplings, or vegetables are present, apply the existing cold source to the damaged area. The entire deltoid area should be in the "cooling" zone. Thus, you will reduce post-traumatic edema in the joint cavity.
Next, you need to immediately deliver the victim to a hospital where there is a traumatologist and an X-ray machine. Before repositioning the dislocation, it is necessary to take a snapshot of the shoulder joint in order to exclude a fracture of the body of the humerus and scapula.

© Andrey Popov - stock.adobe.com
Dislocation treatment
As for how to treat a dislocated shoulder, here are just a few general tips, since self-medication in this case can be very dangerous. The healing process includes several stages:
- dislocation reduction by a qualified traumatologist. Better - under local anesthesia. Ideally, under general anesthesia. Pain relief provides relaxation to muscles that spasm in response to injury. Thus, the reduction will be quick and painless.
- immobilization and ensuring complete immobility of the shoulder joint. The immobilization period is 1-1.5 months. During this period we are trying to achieve maximum healing of the shoulder capsule. For this purpose, in this period, a variety of physiotherapy is prescribed, which helps to improve blood circulation in the affected joint.
- rehabilitation.
We will describe in more detail below the rehabilitation stage in case of shoulder dislocation.

© belahoche - stock.adobe.com. Reduction of dislocation
Rehabilitation
It is necessary to gradually expand the range of motion immediately after removing the immobilization. Despite the fact that the connective tissues have grown together, during the immobilization the muscles weakened and cannot provide the proper stability to the joint.
The first stage of recovery
In the first three weeks after removing the fixation bandage, kinesio tape can be a reliable help, activating the deltoid muscle and thereby increasing the stability of the joint. During the same period, all possible presses and deadlifts should be excluded. Of the available exercises, the following remain:
- Leading a straight arm across the side. The body is fixed in a standing upright position. The shoulder blades are pulled together, the shoulders are pulled apart. Very slowly and in a controlled manner, we move our hand over the side to an angle of no more than 90 degrees. We also slowly return it to its original position.

© WavebreakMediaMicro - stock.adobe.com
- Pronation-supination of the shoulder. The elbow is pressed to the body, the arm is bent at the elbow joint at 90 degrees. The humerus is in place, only the forearm moves. We bring it in and out alternately, with dumbbells clamped in the hand, to the left and to the right. The amplitude is minimal. The exercise is performed until a feeling of warmth arises, or even in the nutria of the shoulder joint.

© pololia - stock.adobe.com
- Flexion of the arms in the simulator, excluding the extension of the injured arm. This is, for example, a block trainer with a built-in Scott bench.
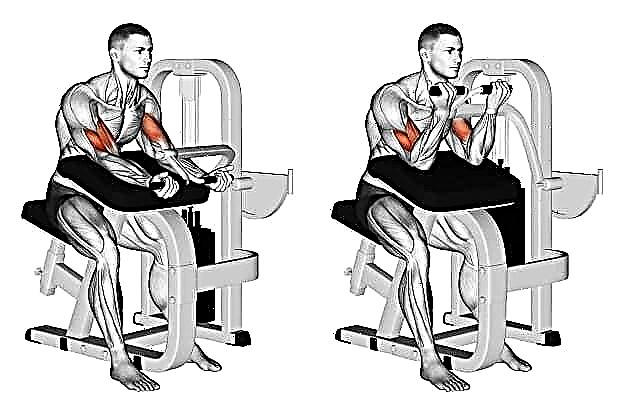
© Makatserchyk - stock.adobe.com
- Extension of the arms in a simulator that simulates the French bench press, the humerus in relation to the body should not be brought out at an angle of more than 90 degrees.



The weight of the burden is minimal, you need to concentrate on the muscle feeling when performing them. Barbells and dumbbells of moderate to heavy weight at this moment are completely prohibited.
Second phase
Three weeks after the removal of immobilization, you can turn on the lifts in front of you and spreading in the slope, to turn on the front and back portions of the deltoid muscle, respectively.

© pololia - stock.adobe.com
We begin to perform spreading through the sides in two versions: with small dumbbells and an extremely clean technique - to strengthen the supraspinatus muscle, and with slightly heavier dumbbells (better in a simulator, but it may not be available in your gym) to influence the middle portion of the deltoid muscle.

© joyfotoliakid - stock.adobe.com

© Makatserchyk - stock.adobe.com
Thus, you need to train for another three weeks. And only after this period, you can carefully return to the usual training regimen, gradually including the pressing and traction movements in the training program. Better - in simulators, with moderate or even light weights.

© Makatserchyk - stock.adobe.com
Push-ups, overhead presses, handstand push-ups and exercises on the uneven bars or pulling out on the horizontal bar or rings are still prohibited. During this period of rehabilitation, which is four weeks long, we gradually increase weights in the pulling and pressing movements, we work mainly on simulators. We pump the deltoid muscles and the muscles of the rotator cuff every workout, preferably at the very beginning.
Stage three
After the four-week stage, you can proceed to work with free weights. It is better to start with a barbell, and only then proceed to work with weights and dumbbells. After mastering the movements with them, you can start working with your own weight again.

© Makatserchyk - stock.adobe.com
Prevention of shoulder dislocation consists in the systematic strengthening of the muscles of the rotator cuff using the exercises described in the first stage of rehabilitation, and working with each muscle bundle separately. Particular attention should be paid to the posterior portion of the deltoid muscle, which is responsible for the stability of the posterior pole of the shoulder capsule.
You should never start training deltas with large weights and bench exercises / D as a warm-up it is very useful to pump each beam separately, perform exercises for the rotator cuff.
Injury Exercise
As it is not difficult to understand from the above, the most traumatic exercises in CrossFit are gymnastic elements performed on the rings and on the uneven bars, snatch, clean and jerk and exercises leading to them, walking and handstand.
However, no exercise will harm you if you approach your activities wisely and in a balanced manner. Avoid one-sided stress, develop your body harmoniously and be healthy!